DOUBLE
CATARACT
- then double vision
the less-than-happy story of a routine operation
Fourteen
months elapsed
between the day my optician decided that my cataracts
were so large as to require surgery
and the day I finally received my next pair
of satisfactory prescription spectacles -
which worked for a while...
If
you are very short-sighted
and require cataract surgery
read this before your first eye
is operated on.
|
Cataract Day Surgery is the commonest planned surgical procedure in the world. When I was told I would need it done on both eyes, I had no qualms at all, despite my distrust of the medical profession in general, and hospital administrations in particular.
In the UK, routine surgery like this involves a long period of waiting, because its National Health Service is geared more to emergency treatments, to expensive amd complicated procedures which are more interesting to surgeons - and (of course) to cancer treatments because of the glory of the 'fight against cancer' and huge public pressure to treat tumours which are largely (but not entirely) a result of the West and North European way of life which afflicts more and more of the world. This way of life involves a great deal of stress, the consumption of huge quantities of meat, refined carbohydrates and sugar, and little natural joy in living. But I digress. Eight months after I was told that my cataracts were large, I went for day surgery to my worse eye - the right eye. Meantime I had been given leaflets on the procedure, which I read carefully, and I had no qualms at all. The operation was performed at my local hospital - a brand-new, depressing and labyrinthine place, obviously designed and built on the cheap to last no more than twenty years - but only 8 km away from my rural home. (I noticed the cheap vinyl on the floors, laid with joins which had shrunk.) It went marvellously well: a painless, very slick and smooth piece of teamwork with plenty of friendly reassurance by all (except, of course, the very handsome young surgeon himself). I was discharged within two hours of my arrival, after liquid refreshment, with my right eye suitably covered. Until recently, cataract operations were performed with general anæsthetic, and patients remained up to two weeks in hospital, forbidden to move their heads more than necessary. I have worn glasses since I was six - that is to say, for 67 years. After the operation I had reasonable monocular vision through their left lens, and I felt that I would have no problem at all while I waited for an unspecified period to have the lens replaced (with a plastic membrane) in the left eye. In this I was sadly mistaken. The notes and advice I was given covered only the strictly medical aspects of cataract day-surgery. I left the hospital with two bottles of drops, instructions on how to use them, and another booklet on coping with life after my little operation. I kept the covering on my eye until the following morning, as recommended. It was when I removed this covering that I was surprised to find that, with my "new" eye the world was not only painfully bright, but very blue. This was due to the fact that my cataracts were rust-coloured, so tended to tinge the world reddishly. The next problem was the fight that started in my brain between what each eye was seeing. This was somewhat disorienting, but, the booklet assured me, the diorientation would not last long. Nevertheless I quickly sawed off most of the plastic in my very thick, rimless glasses, so that each of my eyes would have maximum vision. What the booklet did not mention was the basic law of refraction: light coming into my left eye was refracted by the thick lens and thus came at a different angle to the light which came directly into my right eye. This created a large parallax problem, known as 'refractive error'. Distant vision was affected only slightly, but near vision was poor. Close-up vision was even worse.
The booklet actually recommended that I could continue to wear my old glasses. Even with one lens largely removed, this was a recipe for an Accident In the Home. Nevertheless, I managed to steer myself around the house, and cooked a meal without too many awkward moments involving parallax: pouring liquids, for example. One-eyed people get over this, of course, but only over a long period of being unable to judge the relative positions of tap and kettle, kettle and vessel, vessel and plate. I read a great deal (maybe two or three books a week), and run three websites and four blogs. It was impossible to do this with my two very different eyes. The only solution to this was to use either one of my eyes: the new eye with a magnifier for reading, or the old eye with the bifocal lens of my glasses. The booklet actually recommended the purchase of off-the-peg plastic reading-glasses (commercial objects which I have always believed to be dangerous). So I bought a pair with a two-dioptre magnification, even though I established that my right eye required a 1.75-dioptre magnification. This was not available in the various local suppliers. I blanked off the left eye with black insulation tape. The result was that I could read maybe one or two pages of normal book print, but then my 'new' eye would get very tired and red. I then put a piece of black card over the now-removed right lens of my prescription glasses, so that I could read a bit with my still-cataracted left eye through the bifocal lens. This was not very satisfactory, and soon my left eye suffered strain. I had an almost continuous eye-strain headache.
My various pathetic aids to my surgically-impaired
vision - frequently mislaid
I did not play the usual grateful and subservient patient when I talked to this member of the 'care' team on the telephone. Had I fallen down the stairs or scalded myself on the Friday, Tuesday would have been rather late to do anything, since I live alone in a remote spot…and she probably would not have flagged up an emergency but just shrugged her shoulders, assuming that I was not at home. So I was pretty sharp with this young woman, and I suspect that she may have marked my file DIFFICULT PATIENT - which, I am assured by a friend who is a nurse, is not unusual. It will be no surprise to readers that 'people-skills' in the socially/religiously-divided and divisive cultural desert of Northern Ireland are extremely rare. My own aren't great, and tend to be bipolar... When I asked how long it normally takes for the second cataract to be removed, she told me (truthfully) that it is two to three months. I was dumbstruck. This is utterly outrageous. In other countries with free medical care (France, Germany, Scandinavia, Finland, etc.) the second operation is carried out within 3 weeks (all being well). I had to wait eight months for the first operation (partly because my optician failed to notify my doctor for two months, and then only when my doctor told me that he had not been notified). I won’t have full vision until a year after my cataracts were deemed to need removal. Meantime I could be categorised as VISUALLY IMPAIRED, unable to do some fairly 'normal' things. Two weeks after the operation, I went for a routine check-up. This was not a pleasant experience. In Northern Ireland (if not the entire hitherto United Kingdom) patients are treated like morons - by people with practically no education. Their attitude towards patients’ concerns is exactly as it was in the 1940s when I had a totally unnecessary tonsillectomy. The auxiliary who checked my eyes regarded me with that slight smile indicating stretched toleration of a patient who is, in his field, at least as qualified as her. Nevertheless, my age (71) put me into a category in which I am treated with infuriating condescension bordering on contempt. She told me, however,that my case would be marked Urgent - adding that it could not be the following week (three weeks after the first operation) ! As if there was an ice-cube's chance in Hell of my being moved up the queue so dramatically. Needless to say, my file was NOT marked Urgent. It is certainly the case that the continuously-depleting gene-pool in Northern Ireland (due to the island's main export: intelligent people) means that many patients seem indeed to be semi-moronic. This, however, applies equally to the nursing staff who dealt with me. When I talked of my liking for rural France and the quality of life there (8 on a 10-point scale on which Ireland barely touches 1), one nurse told me of her outrage that people in Brittany did not speak English, and how offensive they were not to keep their shops open during the obligatory and traditional French lunch-break (usually two or three hours) just so that she could buy alcohol to drink with her young friends. My prescription glasses have been for nearly 30 years Reactolite - self-darkening in bright sunshine because of my photophobia. So I had to buy sunglasses to deal with the intolerable increase of light in my right eye. It was not long before I began to regret having the surgery. Better, I thought, to go blind slowly and gracefully, than have to swap various adapted visual aids - which of course I tended to mislay. My confidence began to erode - especially after tripping over a kerb and falling flat on my face. I bumped into things, and had difficult reading notices and documents when the appropriate visual aid was not to hand - or mislaid. I lost a credit card. I cut my toes in mistake for my toe-nails. Three times I was nearly knocked down because cars suddenly appeared out of the mist in my left eye. My confidence eroded further. It is through this kind of experience, unmoderated by non-existent or negative after-care that old people are hastened towards dementia (see below). For the same reason (of panic in the usual cramped and tacky post-office in the usual overlit, brash and noisy tacky supermarket), I dropped my wallet on the street. After several hours of near-despair, I was phoned by a kind shopkeeper to whom some youths had handed it. Whoever compiles the advisory booklets - probably a qualified doctor who has never undergone cataract surgery and who, like most doctors, has little imagination - has not considered that someone who has worn spectacles for 67 years might feel bereft and vulnerable without them. Every morning, on waking, I look around for my glasses. He or she has no interest in colour (and is certainly not a painter) and does not consider that seeing the world blue-tinted with one eye and reddish with the other might be disturbing. Even worse, refractive-error problems when using a keyboard lead to continual mistypying if one is not a touch-typist. But at least screen-text can be enlarged. After my brisk, not to say brusque, check-up I waited to hear when I might have the second eye operated on to match the first. Notice is sent out at least three weeks prior to surgery. It comes, poorly presented and containing acronyms such as "the ICATS team", which, I later discovered, is the pre- and post-surgery team about which I am complaining. After
a month I had heard nothing. So I wrote to the Downe Hospital's
Commanding Officer or CEO or whatever title he glories in -
and received neither acknowledgement nor reply. The normal (or recommended) period between eyes is 3 weeks. Had I not had some intervention, I would have waited three months, with only slightly-diminishing headaches and need to lie for periods a darkened room during the daytime. Thank goodness for BBC radios 3 and 4, and RTÉ Lyric ! I have now even less faith in BritIrish hospitals than I had before. I underwent the completely unnecessary ordeal of having a tonsillectomy when the NHS was first set up. It was horrible: bullying nurses, uneatable sloppy and meaty food on bent tin plates, and a régime for a 6-year old which would not be considered suitable in a prison hospital today.
My globe-trotting mother descended into dementia as a result of someone leaving a swab in her after a ‘routine’ operation for a prolapsed rectum when she was in her late seventies. She nearly died, had to have a colostomy, then submitted to a colostomy reverse: two further general-anæsthetic affairs that completely removed her previously sturdy confidence. It is worth remembering that far, far more people are killed (often slowly and painfully) by doctors than by 'terrorists'. Her sister had her life painfully and callously prolonged (in the same Ulster Hospital) as they kept pumping antibiotics into her for terminal pneumonia, even though she kept saying “I want to die. I want to die”. I once had an unnecessary prostatoscopy which left me with worse Benign Nocturnal Polyuria than before. My prostate remains healthy, if slightly enlarged - as is to be expected. It was not the consultant urologist who told me about BNP - but the internet. He should have diagnosed this at the outset. This was yet another (if very minor) case of routine medical incompetence. Apart from the actual cataract operations I had in Downpatrick (as opposed to the 'ICATS Team' there), the only not-unpleasant experience I have had of a hospital this side of France was when I arranged, of my own volition when I was younger and of indeterminate sexuality, to have a vasectomy, for which I paid very little: just the basic fee to the anæsthetist, and nothing to the sympathetic, antinatalist surgeon. I shall certainly not go into hospital voluntarily again. Preferably for nothing more than an autopsy. I don't like being shunted and abandoned like a railway-wagon. Replacement knee ? forget it! Replacement hip after a 3-year wait - no thank you. Besides, they last only 8-10 years, and I think it somewhat immoral for the old in rich countries to get that sort of operation for nothing, while millions in the world don't even have a lavatory of any kind, much less access to basic medical care and prophylaxy - let alone day-surgery for cataract and glaucoma. Chemotherapy
- absolutely not. DO
NOT RESUSCITATE.
You can see that my right eye (to the left)
is red and tired-looking
What to expect after cataract surgery:
DO NOT BUY NON-PRESCRIPTION READING GLASSES
-
1. Since my vision became a problem, my defective hearing improved, and I had to turn down the volume on live radio and recordings of music. Simultaneously, my not-unpleasant and intermittent tinnitus became louder. 2.
My mother, one of the many rape-victims
on British soil in World War 2, was unfortunately influenced
by two men: her GP brother and her own doctor. Both of these
Royal Navy Surgeons were appalled at my sensitivity as a child,
and persuaded her to send me, at her own considerable expense,
to send me to a private school, which, they said, would This
was of course a disaster from their and her point of view: 3. I am still reaching for my glasses every morning. 4.
After the second eye was eventually treated (one month before
the usual but scandalous three-month wait), the surgeon himself
telephoned me - But I spent up to an hour at times looking and feeling for my crude plastic reading-glasses (recommended even by the RNIB, although they are suitable for only one of my eyes)...feeling stupid and silly and slightly desperate. If I had worn them on a string around my neck they would soon have been crushed. I cannot understand why these cheap and inadequate prostheses are not sold in half-glass (lunette) form. My stability also was restored. I
had to wait six weeks for the left eye to 'settle', before getting
an eye-test By this time, my right eye was extremely tired, I had continuing eye-ache and headache, and deteriorating vision in this 'good' eye. There
could hardly be an easier and surer way |


January 2014
Over one year after my cataracts were deemed to be serious enough
to remove - I finally was able to wear
prescription-glasses again. What a relief! But whereas before, my "good
eye" was the left one,
now my left eye is not good at all, especially for reading.
Whereas I was short-sighted before, I am now long-sighted.
This means that without my glasses, for example in bed, I cannot see
near objects at all well.
The digital clock is even harder to read than it was before I had the
operations.
I guess it's a matter of luck how well the plastic lens has been
inserted into the eye
- or even how well the pre-operation measurements were taken.
My little saga continued even after my post-surgery eye-test,
because the new glasses turned out not darken sufficiently in bright
sunlight.
It turned out that their lenses were of polycarbonate,
which for some technical reason does not darken as much as the plastic
in my previous spectacles.
I am somewhat photophobic, and have had photochromic
lenses for over 20 years.
So they had to go back and be re-made.
October 2014
Over a year since the second operation, I still have some difficulty
with reading,
and, in bed, I still mourn the loss of my short-sightedness.
March 2015 - DOUBLE VISION
My eyesight is actually getting worse, and I am getting peripheral
hallucinations,
and double vision even wearing my glasses,
which I had never experienced before my operations.
July 2015
Returning from France (where I fell at the end of May and broke
my hip,
necessitating a replacement operation
in the Centre Hospitalier, Villefranche-de-Rouergue) ***,
I visit my optician to find out if I am imagining my decrease in vision.
He tells me that I have posterior capsule opacification in both eyes.
The following is from the Royal National Institute for the Blind's website:
Cataract surgery is generally very successful.
Only about three per cent of people who have cataracts experience complications.
The most common complications can be dealt with and usually don't affect
sight in the long term.
One
of the most
common complications is a thickening of the lens capsule
which holds the lens in place.
This may occur a couple of months or even years after the original operation.
If this happens, your sight will become cloudy again, as though the
cataract has come back.
Doctors call this complication posterior capsule opacification
or posterior capsule thickening
and it is usually easily dealt with by a small laser operation done
through an outpatient appointment.
*** In France I had pretty good treatment: a room to myself (which is
normal) with a pleasant view,
an excellent surgeon, variable nursing staff whose attitudes ran the
gamut from arrogant
(the youngest) to friendly and humorous (the males and older females),
and appalling food, completely un-nourishing and lacking in vitamin
C
(while high in salt, additives and sugar) and reminiscent of a British
canteen or school from the 1950s
- but presented with plastic and cling-film. Half of it went down the
WC.
Not a single salad was offered during my 8-day stay.
I encountered the same lack of information as in Northern Ireland.
There seemed to be no general policy of telling the patient what to
expect.
It wasn't until I talked to a physiotherapist at the Downe Hospital
that I learned that I might still have difficulty in walking in 4 months'
time.
I was allowed to believe in France that I would be walking well in 8
or 10 weeks,
and I was not told, for example, how best to get into a car - one of
the most difficult actions
and one which nowadays is 'rudimentary'.
November 2015
I finally had an appointment at the eye clinic of the Mater Infirmorum
Hospital in Belfast,
which appeared to be in a state of permasnent chaos - more like an Emergency
Unit than an eye clinic.
Doctors were rushing around in and out of small rooms; machines were
breathlessly used by one,
then another. I did not expect to get out of this place with my sight
improved.
However, after being in and out of rooms and corridors, my left
eye finally received the laser treatment.
But they did nothing to my right eye, because, one of the doctors told
me, they thought I had
Age-related
Macular Degeneration.
I would need an appointment at the Macular Clinic of the same hospital.
My left eye was immediately restored to excellent vision.
But my right eye got gradually worse, my vision fuzzier,
as I awaited an appointment to find out whether my A.M.D. was 'wet'
or 'dry'.
February 2016
The Macular Clinic, in "temporary" huts just across
the road from the Eye Clinic, turned out to be much less chaotic,
and the staff very friendly, respectful and charming for the first time
in this long saga.
My medical history is gone through yet again. My eyes are scanned
and examined several times,
and I am eventually told the good news: I do not have Macular Degeneration.
This was a mis-diagnosis across the road, and I should have received
the laser treatment on my right eye
back in November.
However, a membrane is growing over the retina of both eyes,
and it is slightly wrinkled.
This has several names, amongst which is Macular
Pucker.
Although this is causing no problem at all at the moment (as I said,
my left eye is fine)
it could get thicker and require removal by surgical intervention.
This delicate and sometimes-successful surgery I will certainly
not undergo - at least not in the "United Kingdom".
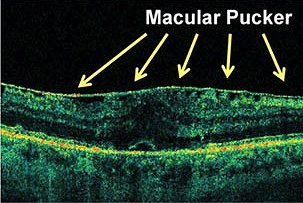 |
This is the
less than informative picture which I was shown at the Macular
Clinic in Belfast. |
Further bad news is that there is no YAG-laser machine in the
Macular Clinic.
The system does not allow them to lift a phone or give me a little chit,
or to carry my file across the road to get the 10-minute laser treatment.
I shall have to wait at least another month to receive notice
to make an appointment
which will be at least three weeks after that.
April 2016
I go to a very new "Wellbeing Centre" (also in Belfast)
which to my delight is not a 'temporary' erection,
nor an overcrowded Victorian corridor, but like a clinic one might find
in France - a quiet,
well-designed, non-'sick' building, where I meet a charming chap who
does the preliminaries,
then brings me to the consultant, a sensitive and concerned woman
who has just driven the 50 kms from the hospital close to where I live,
the hospital where I had the cataract operations and which has no YAG-laser
machine.
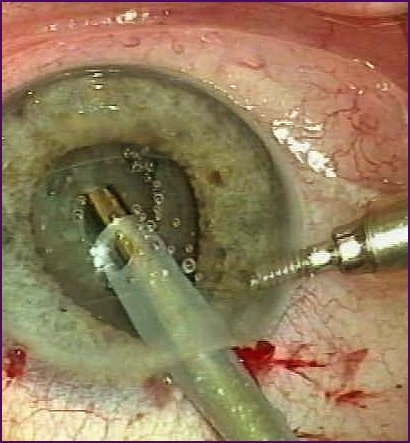
Within ten minutes the opacity in my right eye has gone, and
I can see clearly again
- for a time - with both eyes.
HALLELUJAH!
(Though the right eye now sees significantly better than the left
eye, both with and without glasses.
Do I need another eye-test ?)
August 2018
By now I am having problems with my left eye. I got an appointment
with the local eye clinic (mere opticians
do not do eye-testing or diagnosing in France), who referred me to their
main clinic in the 'County Town' of Montauban.
This place was remarkably efficient. Within ten minutes of
the appointment time I am seen by clinician number 1.
Then I wait another 10 minutes to be seen by clinician number 2. Then
number 3 - and finally the chief honcho
who tells me that a membrane is growing over both my retinas, but especially
in the left eye. He tells me that previous treatment had been pretty
ham-fisted. I am given a date for another examination in three months.
November 2018
I go through the same procedure again, this time with only
3 examinations,
and am given an appointment there and then for outpatient surgery in
a fortnight's time.
I receive a folder of advice and information.
The surgeon will "clean out" the eye and remove the retinal
membrane.
I will be able to leave the clinic soon after,
but improvement in vision may be slow- - or even negligible.
In fact, improvement in vision was immediate, as if a veil
had been lifted.
I entered the Clinique Honoré Cave in Montauban at 09.30 and
left at 12.30 having had a very pleasant time.
The surgeon told me at the end of this operation that she had done a nice job.
I was given a sheet telling me exactly what was done, including
pre-disinfection, suturingand colour staining.
Here is the important bit: after removing the vitreous humour of the
eye,
the surgeon performed a bit-by-bit removal of the chunk of epi-macular
membrane which was growing over the retina,
and similarly of the internal limiting membrane (which had previously
been stained to make it show).
Then the eye was flushed out, and sutured, the vitreous humour replaced
with saline solution...
A régime of drops 3 and 4 times a day continue for a period.
|
|
|
this site only |